Primitive Reflexes and Your Child’s Development
When hearing the word “reflexes,” most people recall sitting on crinkly paper at the doctor’s office while a physician taps a knee with a little rubber mallet. The leg kicks out, and everyone nods as if something profound just happened. It serves as a funny little ritual. People tend to think reflexes are just automatic quirks that prove nerves are working. However, when looking at children, reflexes play a much more critical role than just making a leg kick straight. They are actually the building blocks of almost every movement and skill a child will develop.
Occupational therapists look at specific movement patterns called primitive reflexes. These include the Moro Reflex, Asymmetrical Tonic Neck Reflex (ATNR), Symmetrical Tonic Neck Reflex (STNR), and the Tonic Labyrinthine Reflex (TLR). These names might sound like a foreign language right now. However, they are actually fascinating keys that unlock why a child moves, behaves, and learns the way they do. When these reflexes do not fade away or “integrate” at the right time, they can cause a domino effect of challenges.
Eyas Landing sees these challenges every day. The team also sees the incredible progress children make when addressing them. Eyas Landing meets families where they are, whether that is in the home, at the clinic in the West Loop, or through telehealth. The goal is to help parents make sense of these reflexes so they can support their child in the best way possible.

What Are Primitive Reflexes?
Think of primitive reflexes like the training wheels on a bicycle. When a baby is born, their brain is not quite ready to control every single muscle consciously. So, nature provides a set of automatic movements to help them survive and start moving. These are primitive reflexes. They originate in the brainstem, which is the part of the brain responsible for basic survival functions.
These reflexes help a baby take their first breath, grasp a finger, and eventually lift their head. They are essential for the first few months of life. However, just like training wheels, there comes a time when they need to come off. As a baby grows, their higher brain centers should take over. The automatic movements should fade away to make room for voluntary, controlled movements. This process is called integration.
When a reflex integrates, it merges into more complex movements. It becomes part of the background operating system. However, sometimes these reflexes stay active longer than they should. This is called a “retained” reflex. When a reflex is retained, it acts like a glitch in the software. The child has to work extra hard to override the automatic movement. This can lead to fatigue, frustration, and difficulties with things like reading, writing, sitting still, and even regulating emotions.
 The Moro Reflex: The Alarm System
The Moro Reflex: The Alarm System
The Moro Reflex is often called the startle reflex. Parents have likely seen this in a newborn. If a loud noise occurs or their head drops back suddenly, the baby throws their arms and legs open wide and takes a sharp breath. It is an automatic fight-or-flight response. It acts as an internal alarm system designed to alert the baby to potential danger.
This reflex appears at birth and should typically integrate between two and four months of age. It serves a great purpose for a tiny infant who cannot protect themselves. However, imagine if that alarm system never turned off. Imagine walking through the day with a fire alarm ringing in the ears every time a door slammed or a light flickered. That is what life feels like for a child with a retained Moro Reflex.
If this reflex is not integrated, a child remains in a constant state of hypersensitivity. Their body reacts to the world as if everything is a threat. Parents might notice that their child is hypersensitive to changes in their environment. They might cover their ears at loud noises that do not bother others. They might have a strong dislike for tags in their clothes or certain textures of food.
These children often struggle with anxiety because their body is constantly flooded with stress hormones like cortisol and adrenaline. This can lead to poor social skills because they are too busy scanning for danger to interact with peers. Adults might see poor impulse control or emotional outbursts that seem to come out of nowhere. It is not that they want to misbehave. Their body is simply reacting to a perceived threat.
Fatigue is another major sign. Being on high alert all day is exhausting. After a day at school, these kids might come home and completely crash or have a meltdown. They might also suffer from motion sickness or have poor balance. Integrating the Moro Reflex helps turn down that internal alarm dial. It allows the child to feel safe in their body and their environment.
 Asymmetrical Tonic Neck Reflex (ATNR): The Fencer
Asymmetrical Tonic Neck Reflex (ATNR): The Fencer
The Asymmetrical Tonic Neck Reflex, or ATNR, is often recognized by its classic pose. When a baby turns their head to one side, the arm and leg on that same side extend straight out, while the arm and leg on the opposite side bend. It looks a bit like a fencer getting ready to lunge.
This reflex is crucial for the birth process and helps the baby make its way down the birth canal. In the early months, it prevents the baby from rolling over before they are ready. It also helps start the connection between the eyes and the hands. The ATNR appears at birth and should ideally integrate by six months of age.
The ATNR defines the sagittal midline. This is an imaginary line that runs down the center of the body, dividing left from right. Integration of this reflex allows a child to cross that midline with their hands and eyes. It facilitates rolling, crawling, and reaching. It influences eye-hand coordination and horizontal eye pursuits, which are the smooth eye movements needed for reading.
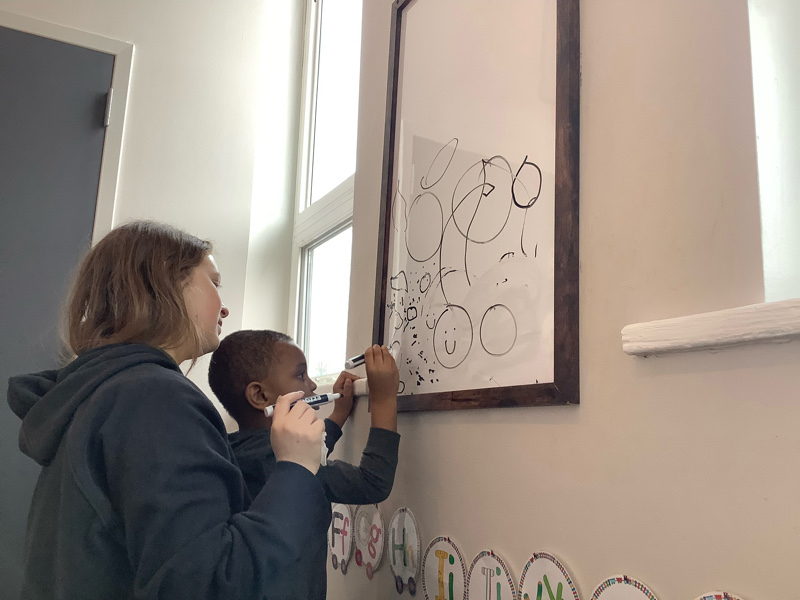
When the ATNR remains active, it causes physical and academic hurdles. A child might have difficulty crossing the midline. This means if they are holding a crayon in their right hand, they might stop drawing when they reach the middle of the paper and switch hands. This interrupts the development of a dominant hand. Parents might notice their child uses both hands equally but not skillfully.
Handwriting is often a major struggle. Every time the child turns their head to look at the blackboard, their arm might want to straighten involuntarily. They have to use a lot of mental and physical energy just to keep their arm bent and holding the pencil. This leads to a tight, awkward pencil grip and messy writing.
These children might also struggle with balance and bilateral coordination, which is the ability to use both sides of the body together. Activities like riding a bike, catching a ball, or even marching can be difficult. They might seem clumsy or uncoordinated in sports. Integration of the ATNR is vital for smooth, rhythmic movement and academic success.
 Symmetrical Tonic Neck Reflex (STNR): The Crawler
Symmetrical Tonic Neck Reflex (STNR): The Crawler
The Symmetrical Tonic Neck Reflex, or STNR, is the bridge to crawling. It helps the baby learn to use their upper and lower body independently. When the baby lifts their head, their arms straighten and their legs bend. When they lower their head, their arms bend and their legs straighten. It is like a little push-up mechanism.
This reflex appears a bit later, usually between six and nine months, and should integrate between nine and eleven months. It is a short-lived reflex, however it serves a powerful purpose. It helps develop muscle tone in the neck and upper back. It also assists with visual accommodation, which is the ability to change focus rapidly from near to far distances.
A child with a non-integrated STNR often skips crawling on hands and knees. They might “bear walk” on hands and feet or scoot on their bottom. Because they missed that crucial crawling phase, they may not have fully developed the connection between their eyes and their hands.
In the classroom, these children often have terrible posture. They might slump over their desk or prop their head up with their hand because their back muscles are tired. Teachers might see them sitting in a “W” position on the floor, with their legs bent back on either side of them. This position provides a wider base of support so they do not have to use their core muscles. However, it can be bad for their hip joints and core strength in the long run.
The STNR is closely linked to attention and focus. If a child has to concentrate hard just to sit up straight, they have little brainpower left to listen to the teacher. They might be labeled as fidgety or easily distracted. Visual accommodation issues can make copying from the board a nightmare. The constant head movement up and down triggers the reflex, causing their body to want to shift and wiggle.
 Tonic Labyrinthine Reflex (TLR): The Gravity Sensor
Tonic Labyrinthine Reflex (TLR): The Gravity Sensor
The Tonic Labyrinthine Reflex, or TLR, is all about gravity and head position. It is responsible for a child knowing where their head is in space and being able to separate head movements from body movements. It helps a child develop balanced muscle tone and the ability to grade their movements, which means using just the right amount of force.
The TLR appears in utero, which means it is present before the baby is even born. It has two phases: forward and backward. In the forward phase, when the baby’s head tilts forward, their body curls into a ball. In the backward phase, when the head tilts back, the body extends and stiffens. This reflex should be integrated gradually and is usually fully integrated by three and a half years of age.
Because the TLR is so deeply connected to the vestibular system (the sense of balance), it has a massive impact on how a child moves through the world. If the TLR is not integrated, the child is constantly fighting gravity.
The TLR Pose and Posture
One can often spot a retained TLR by looking at how a child stands and sits. If the reflex is still active, the movement of the head dictates the muscle tone of the entire body. When the child looks down to read or write, the forward TLR reflex kicks in, causing their upper back to round and their legs to want to straighten or curl. They end up hunched over their desk.
Conversely, if they look up, the backward TLR reflex triggers. Their back arches and they might tend to lean back or even tip their chair over. This constant push-and-pull affects their postural control. They might appear to have low muscle tone, often described as “floppy.” They might lean against walls, furniture, or other people because holding themselves upright is exhausting.
Toe Walking and Balance
A retained TLR is a common culprit behind toe walking. The extension pattern caused by the reflex can create tension in the calf muscles, pulling the heels up. Walking on toes changes the center of gravity and affects the alignment of the hips and spine.
Decreased body awareness is another side effect. These children might bump into things frequently or have trouble judging distances. They might not know where their limbs are without looking at them. This leads to that “bull in a china shop” phenomenon.
Ocular Motor Control and Motion Sickness
The TLR is tightly wired to the eyes. Stable vision requires a stable head. If the head moves every time the eyes move, or if the body moves every time the head moves, the visual world becomes shaky. This leads to poor ocular motor control. Tracking a line of text across a page becomes a Herculean task. The words might seem to jump or float.
This instability often results in motion sickness. Car rides can be a misery for children with a retained TLR. They might also dislike playground equipment that spins or swings because their vestibular system gets overwhelmed easily. They prefer to keep their feet firmly on the ground.
Coordination and Sequencing
The TLR helps separate body parts to move them independently. When it is retained, the body wants to move as a rigid unit. This makes activities requiring coordination, timing, and sequencing very difficult. Learning to ride a bike, swim, or dance can be frustrating. They might struggle to follow multi-step physical instructions because their body simply does not want to cooperate.
 Why Integration Matters
Why Integration Matters
Parents might wonder what happens if these reflexes never integrate. If a child’s reflexes are not fully integrated, they may never disappear on their own. The body is a master of adaptation. It will find workarounds. The child will develop compensatory strategies to get by. They might learn to grip the pencil tighter to control the wobble. They might learn to avoid sports to avoid the embarrassment of clumsiness.
However, these compensations come at a cost. They require immense energy. A child who uses eighty percent of their energy just to sit still and hold a pencil has only twenty percent left for learning. This is why teachers often see smart, capable children struggling in school. It is not a lack of intelligence. It is a lack of neural foundation.
With changes in their lives, the affects that the non-integrated reflex has on their skills will change. A retained reflex that caused feeding issues as a baby might cause anxiety as a teenager. The symptoms shift, however the root cause remains the same.
The good news is that the brain is plastic. It can change and learn at any age. Occupational therapy can help integrate these reflexes through specific movements and exercises. This process is often called “re-patterning.” It gives the brain a second chance to go through those early developmental stages.
How Eyas Landing Helps
Eyas Landing looks at the whole child. The focus is not just treating the symptom; it is about looking for the underlying cause. The occupational therapists are experts in assessing primitive reflexes. They use a combination of standardized tests and clinical observations to see which reflexes might be playing a role in a child’s challenges.
Flexibility is the foundation of the approach to pediatric therapy. Eyas Landing knows that a clinic setting is great for some things, however sometimes seeing a child in their natural environment gives better clues. Therapists can observe how they sit at the dinner table at home or how they manage the playground at school.
Therapists collaborate across disciplines. An occupational therapist might work with a physical therapist to address the gross motor issues caused by a retained TLR. They might work with a speech therapist if the ATNR is affecting the child’s ability to coordinate the muscles for speech. Eyas Landing treats the entire family, not just the child. When one family member struggles, everyone feels it.
The team creates a treatment plan that includes activities to help integrate reflexes. These are often simple, rhythmic movements that can be done at home. This is called a “sensory diet” or a home exercise program. Parents are taught these strategies so they can be an active partner in their child’s progress. The goal is for parents to feel confident in helping their child.
For example, to help integrate the TLR, activities might challenge the child to curl up like a ball and then extend like a superhero against gravity. Therapists might use swings or therapy balls to stimulate the vestibular system. For the ATNR, they might do “lizard crawls” or activities that require crossing the midline.
Compensatory strategies are also taught. While working on integrating the reflex, making life easier right now is also important. This might mean using a slanted writing surface to help with head position or providing a special seat cushion to improve posture. The focus is on increasing overall success and independence within the completion of activities of daily living.
Signs Your Child Might Have Retained Reflexes
If reading this causes nodding heads, parents might be wondering if their child has retained reflexes. Here is a quick checklist of things to watch for. Remember, every child is unique, and having one or two of these does not definitely mean there is an issue. However, if a cluster of these signs appears, it is worth looking into.
Possible Signs of Retained Moro Reflex:
- Easily startled by loud noises or sudden movements.
- Anxiety or fearfulness that seems disproportionate to the situation.
- Difficulty with transitions or changes in routine.
- Motion sickness.
- Poor stamina or quick to fatigue.
- Emotional outbursts or mood swings.
Possible Signs of Retained ATNR:
- Poor handwriting or a tight pencil grip.
- Difficulty with reading, especially tracking across the page.
- Confusion between left and right.
- Difficulty catching a ball or riding a bike.
- Tendency to use one side of the body more than the other.
Possible Signs of Retained STNR:
- Poor posture or slouching.
- “W” sitting on the floor.
- Messy eating habits.
- Difficulty copying from the blackboard.
- Poor attention and focus.
Possible Signs of Retained TLR:
- Toe walking.
- Poor balance or clumsiness.
- Fear of heights or excessive risk-taking (poor danger awareness).
- Motion sickness.
- Difficulty with sequencing and timing.
- Muscle tone that seems too stiff or too floppy.
Moving Forward with Hope
It can be overwhelming to realize that something as automatic as a reflex could be the source of so much struggle. However, it is also incredibly hopeful. It means that the challenges a child faces are not because they are “lazy” or “difficult.” There is a physiological reason behind it. And more importantly, there is something that can be done about it.
Recognizing these signs is the first step. The next step is taking action. Families do not have to figure this out alone. The team at Eyas Landing is here to guide the way. They have the expertise to assess these reflexes and the creativity to design a plan that works for specific families.
Success stories happen every day. Children who used to hate writing suddenly start drawing for fun. Kids who were terrified of the swings start asking to go to the park. Anxiety decreases and confidence soars. It is not magic. It is neurology. It is the power of giving the brain the strong foundation it needs.
Every child has so much potential waiting to be unlocked. Addressing primitive reflexes is often the key that opens the door. If concerns exist about a child’s development, trust that instinct. Parents know their child better than anyone.
For more information, please reach out to an occupational therapist. If one is not already in place, Eyas Landing is here to help. An evaluation can be scheduled to look at these reflexes and see how to support a child’s journey. Let us work together to build a strong foundation for future success.
“Eyas” is defined as a young hawk in the developmental stage of learning to fly. At Eyas Landing, it’s not only
about the flight, but also the landing. “As our clients succeed in therapy, they succeed in every aspect of their daily life.”- Dr. Laura Mraz, OTD, OTR/L Founder of Eyas Landing since 2007
Three Birds. One Mission.
Eyas Landing is just one part of your child’s journey! Our sister companies, Blue Bird Day and Merlin Day Academy, work together to support your child as they grow. Blue Bird Day, our therapeutic preschool and kindergarten program, is an intensive rotational therapeutic program designed to provide children ages 2-7 with the tools they need to succeed in a classroom environment. Merlin Day Academy— accredited by the Illinois State Board of Education—provides special education and multi-disciplinary therapy for children ages 6-14 with neuro-diverse learning needs.


Eyas Landing is a therapy clinic with a mission to provide evidence-based and family-centered therapy services for children, adolescents, and their families. The primary goal is to deliver relationship-based interventions within the most natural environments and to empower families to reach their full potential. To achieve this goal, our highly educated, compassionate staff dedicates time and expertise to create experiences that maximize therapeutic outcomes. The strength, determination, and perseverance of our clients are evident as they succeed in therapy, and ultimately in their daily lives.
Eyas Landing offers a wide range of comprehensive services including Speech Therapy, Occupational Therapy, Physical Therapy, ABA Therapy, Social Work, Family Therapy, and Neuropsych testing. Services are provided throughout the Chicagoland area via Telehealth, In-Home, and in our state of the art clinic.
Want to learn more or you have a specific question? Feel free to connect with us here!